Endometriosis
Endometriosis is a common health problem in women that occurs when cells or tissue from the lining of the womb (uterus) grows outside the uterus, on other organs or structures in the body. Most often, endometriosis is found on the: Ovaries, Fallopian tubes, Tissues that hold the uterus in place (uteroscaral ligament), Outer surface of the uterus, Lining of the pelvic cavity. Other sites for growths can include the vagina, cervix, vulva, bowel, bladder, or rectum. In rare cases, endometriosis has been found in other parts of the body, such as the lungs, brain, and skin.
Endometriosis sometimes runs in the family and you are more likely to develop endometriosis if you: started your period at a young age, never had children or have frequent periods or they last 7 or more days
The pain of endometriosis can interfere with your life. Studies show that women with endometriosis often skip school, work, and social events. This health problem can also get in the way of relationships with your partner, friends, children, and co -workers. Plus, endometriosis can make it hard for you to get pregnant. Finding out that you have endometriosis is the first step in taking back your life. Many treatments can control the symptoms. Medicine can relieve your pain. When endometriosis causes fertility problems, surgery can boost your chances of getting pregnant.
Why does endometriosis cause pain and other problems?
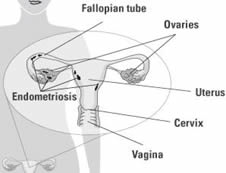
Each month during the menstrual cycle, the ovaries produce sex hormones that build up the lining of the uterus (womb) with tissue and blood vessel, such that the lining of the womb (endometrium) swells and become thicker. If a woman does not get pregnant during that cycle, the uterus sheds this tissue and blood. It comes out of the body through the vagina as her menstrual period, or quite often flows back into the pelvis, through the fallopian tubes (see diagram)
The endometriosis tissues (located outside the womb) behave exactly like that of the normal lining of the womb, in that it responds to the sex hormones and become built up, with swollen and thicker tissue and blood vessels during the menstrual cycle. However, unlike the endometrial cells found in the uterus, the tissue implants outside the uterus are unable to freely release menstrual bleeding, so they stay in place – trapped and under tension – during the period and for longer, (although a small amount may leak out or be absorbed back into the the body). This happens again at the next period; and it is this repeated process that leads to pain and other symptoms of endometriosis, due to the build up and expansion of trapped tissue and blood – continously stretching the nerves endings for pain. Tissue and blood that is leaked into the body also can cause inflammation, scar tissue, and pain. As endometrial tissue grows, it can cover or grow into the ovaries and block the fallopian tubes. Trapped blood in the ovaries can form cysts (endometrioma or endometriotic cyst). It also can cause inflammation and cause the body to form scar tissue and adhesions, tissue that sometimes binds organs together. This scar tissue may cause pelvic pain and make it hard for women to get pregnant. The growths can also cause problems in the intestines and bladder.
What Causes Endometriosis ?
The cause of endometriosis is unknown, but experts have a number of theories.
- One theory is that the endometrial cells shed when the menstrual flow travel backwards through the fallopian tubes into the pelvis, where they implant and grow. This is called retrograde menstruation. This backward menstrual flow occurs in many women, but experts think the immune system may be different or faultly in women with endometriosis. Similarly, endometrial tissue has been found in abdominal scars and might have been moved there by mistake during a surgery. If a woman has a faulty immune system it will fail to find and destroy endometrial tissue growing outside of the uterus. However, most experts agree that this theory does not entirely explain why endometriosis develops, as endometriosis tissue, probably carried through the body fluid system, has been found in distant organs, such as in the lungs.
- Since endometriosis runs in families, it may be passed on in the genes, or some families have traits that make them more likely to get it.
- New research shows a link between dioxin exposure and getting endometriosis. Dioxin is a toxic chemical from the making of pesticides and the burning of wastes. More research is needed to find out whether man-made chemicals cause endometriosis.
Symptoms
The most common symptom of endometriosis is pain in the lower abdomen or pelvis, or the lower back, mainly during menstrual periods. The amount of pain a woman feels does not depend on how much endometriosis she has. Some women have no pain, even though their disease affects large areas. Other women with endometriosis have severe pain even though they have only a few small growths. The lower abdominal pains occurs as cramps, and may start for about a week before menstruation, but gets worse, as the periods starts and continues throughout the period. The pain often involves the lower back and pelvis and may occur outside of the menstrual period. Other
symptoms of endometriosis can include:
- Pain during or after sex
- Painful bowel movements or painful urination during menstrual periods
- Spotting or bleeding between menstrual periods
- Diarrhea, constipation, bloating, or nausea, especially during menstrual periods
Diagnosis
The information you provide to your doctor or gynaecologist about your menstrual period and the nature of the pelvic pain that you have will help your doctor to suspect that you may be suffering from endometriosis. An abdominal and vaginal examination – may reveal that you are generally tender in both areas. A painful swelling may be felt, if you have developed cyst of the ovary from the endometriosis; occasionally cysts will be felt on both ovaries. The examination may also reveal the presence of a firm nodule from the scarring of endometriosis.
Tests that are done to help diagnose endometriosis include and pelvic ultrasound, which may be done through the lower abdomen or through the vagina – transvaginal ultrasound. Unless your doctor starts you on treatment, such as the contraceptive pills, on the basis of the assumption that you have endometriosis, from the information you give, it is most likely that a laparoscopy will be necessary to make a certain diagnosis – this is an operation to pass telescopic camera through your belly-button (navel), to have a view of the internal organs on the pelvis. Magnetic resonance imaging (MRI) is another common imaging test that can produce a picture of the inside of your body. This is increasingly showing features of endometriosis quite accurately. In cases where a laparoscopy may be considered, as dangerous or unadvisable, an MRI may be considered first. When laparoscopy is done, if your gynaecologist is experienced in this area, a small sample of the endometriosis may be removed for testing – laparoscopic biopsy of endometriotic deposit. Quite often some surgical treatement will also be carried at the same time, if this was agreed prior to going for the procedure.
Treatment
Treatment of endometriosis depends on the age, severity of symptoms, severity of the disease and whether there are future plans to get pregnant. There is no cure for endometriosis, but there are many treatments for the pain and infertility resulting from this condition:
Pain medication. For some women with mild symptoms, simple pain killers such as ibuprofen, naproxen or acetaminophen (Tylenol), taken only during the menstrual periods, often starting just before may be all that is necessary to keep the symptoms under control. If painkillers alone are being used, and future pregnancy is desired, it is often suggested that a regular check, every 6-12 months is carried out to ensure that the endometriosis is not getting worse. If simple pain-killers are not effective, your doctor may prescribe stronger ones.
Hormone treatment. Hormonal treatments are often recommended to treat endometriosis, if simple analgesics are ineffective or to stop the endometriosis from getting worse. Only women who do not wish to become pregnant can use these medications. Hormone treatment is best for women without endometriosis cyst and do not have severe pain or disease. Medical treatment does nor reverse the changes that have already occured due to the scarring. Common hormones used for endometriosis include:
- Combined Contraceptive Pills prevent ovulation and prevent overgrowth of endometrial tissue, thus reducing the amount of menstrual flow. They contain two hormones, oestrogen and progestogen. Using the pills, non-stop, without the seven days free period, for three cycles at a time, can help to shrink the growth of endmetriosis tissue. However stopping these pills often cause the symptoms of endometriosis to return.
- The hormone progesterone, used continuously can shrink spots of endometriosis by working against the effects of oestrogen on the tissue. Injection of Medroxyprogesterone (Depo-Provera) is a common progestogen formulation used for its ability to also stop the menstrual period, but has side -effects, such irregular weight gain, depressed mood, delayed return of fertility and decreased bone growth. The Mirena Intra-uterine system (coil) containing levonorgestrel is increasing being used for the treatment of endometriosis.
- GnRH analoguesg buserelin, goserelin, are injections which limits the ability of the ovaries to produces the sex hormones, thus reduce the amount of oestrogen and
progesterone, which stops the menstrual cycle. These medications have side effects similar to those during menopause, such as hot flashes, bone loss, and vaginal dryness. Therefore they are not usually recommended alone, for long period of use, unless low dose of oestrogen and progesterone are taken – usually in the form of hormone replacement therapy (HRT) preparations or even as lose-dose combined oral contraceptive pills. After stopping this medication, it is possible to get pregnant. In addition, if used form 6 -9 months, the symptoms of endometriosis often do not come back for months or years afterward, unless there are complications, such as endometriosis ovarian cysts.
- Danazol is a weak male hormone that lowers the levels of oestrogen and progesterone in a woman’s body. This stops a woman’s period or makes it come less often. It is not often the first choice for treatment due to its side effects, such as oily skin, weight gain, tiredness, smaller breasts, and facial hair growth. The side -effects depends on the dosage of medication, therefore its use as a low -dose formulation, may reduce these unwanted effects. As it does not prevent pregnancy and can harm a baby growing in the uterus, if unexpected pregranancy were to result. It also cannot be used with other hormones, such as birth control pills.
Surgery. Surgery is usually the best choice for women with severe endometriosis as there are widespread deposits within the pelvis, there is severe lower abdominal pain, affecting day to day life and in addition there are usually problems with fertility. There are both minor and more complex surgeries that can help. Your doctor might suggest one of the following:
- Laparoscopy can be used to diagnose and treat endometriosis. During this surgery, doctors remove the endometriosis implants and scar tissue (adhesions) or burn them away. The goal is to treat the endometriosis without harming the healthy tissue around it. Women recover from laparoscopy much faster than from major abdominal surgery.
- Laparotomy that involves a much larger cut in the abdomen than with laparoscopy. This allows the doctor to reach and remove growths of endometriosis in the pelvis or abdomen.
- Removal of Both Ovaries +/- Hysterectomy is a surgery in which the gynaecologist removes both oaveries and usually also the the uterus. Removing the ovaries help ensure that endometriosis will not return. This is done when the e ndometriosis has severely damaged these organs. Any scarring can also be divided at the same time. A woman
cannot get pregnant after this surgery, so it should only be considered as a last resort. However, the removal of the womb, fallopian tubes and both ovaries gives the best chance for a cure. Rarely, the condition can return, if there are other sources of oestrogen.
Long-term Concerns
- Long-term (chronic) pelvic pain that interferes with social and work activities
- Large cysts in the pelvis (called endometriomas) that may break open (rupture)
In a few rare cases, endometriosis deposits and/or adhesions may cause blockages of the gastrointestinal or urinary tracts. Very rarely, cancer may develop in the areas of endometriosis after menopause.








Leave a Reply
Want to join the discussion?Feel free to contribute!